Biologie cellulaire
Les péroxysomes
Découvrez les peroxysomes, des petits organelles cellulaires clés pour la survie et l'adaptation de nos cellules ! À travers ce cours de biologie cellulaire, vous ex...
Arthrologie, ou syndesmologie
En pénétrant dans l'étude des articulations humaines, ce cours vous fera découvrir le joint de la hanche, un élément clé du système locomoteur. Explorons les structures qui la constituent et les mouvements qu'elle permet. Développons également notre compréhension des pathologies qui peuvent affecter cette articulation cruciale.
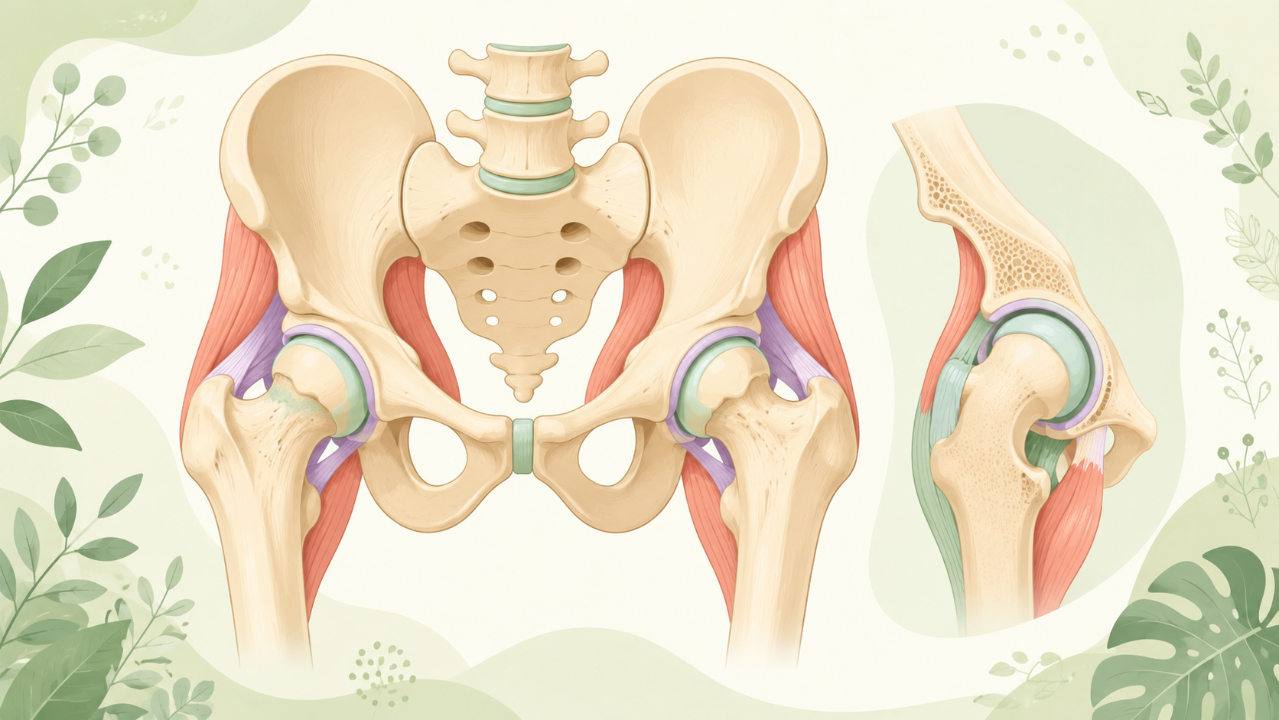
L'articulation de la hanche, ou articulation coxo-fémorale, est l'une des articulations synoviales les plus volumineuses et les plus robustes du corps humain. Elle constitue une articulation sphérique reliant le bassin (acétabulum) au fémur (tête). L'articulation de la hanche permet une large gamme de mouvements, notamment la flexion, l'extension, l'abduction, l'adduction, la rotation interne et la rotation externe. Cet article explore en profondeur l'anatomie, le développement, la biomécanique, les pathologies et les aspects cliniques liés à l'articulation de la hanche.
Les éléments osseux qui composent l'articulation de la hanche comprennent l'acétabulum (partie du bassin) et la tête fémorale. L'acétabulum est une cavité profonde en forme de coupe formée par l'ilion, l'ischion et le pubis. La tête fémorale est l'extrémité arrondie du fémur située au-dessus du col.
La surface articulaire de l'acétabulum est tapissée de cartilage hyalin qui recouvre le bourrelet de la cavité osseuse. La surface articulaire de la tête fémorale est également recouverte de cartilage hyalin, qui s'articule avec le bourrelet et la cavité acétabulaires.
Plusieurs ligaments assurent la stabilité de l'articulation de la hanche, notamment :
L'articulation de la hanche se développe à partir de trois tissus embryonnaires : le mésoderme somatique, le sclérotome et le mésoderme de la plaque latérale. À la fin de la 5e semaine, le bourgeon du membre inférieur apparaît comme une excroissance de l'extrémité caudale du corps. Le fémur et le bassin se différencient et forment l'articulation de la hanche au cours des semaines suivantes.
L'amplitude de mouvement de l'articulation de la hanche est essentielle à la locomotion, au maintien de la posture et aux autres activités quotidiennes. Les principaux muscles responsables des mouvements de la hanche sont :
Les blessures de la hanche peuvent résulter de chutes, d’accidents sportifs ou d’activités à fort impact. Les blessures courantes incluent :
L’arthrose (OA) est la maladie articulaire la plus courante, caractérisée par une dégénérescence du cartilage articulaire, des modifications de l’os sous-chondral et la formation d’ostéophytes. Les facteurs de risque de développement de l'arthrose de la hanche comprennent le vieillissement, l'obésité, la génétique et les antécédents de blessures articulaires.
La DDH est une maladie congénitale ou développementale caractérisée par une instabilité de l'articulation de la hanche due à un développement acétabulaire anormal. Un dépistage et un traitement précoces sont essentiels pour prévenir d'autres complications telles que l'inégalité de longueur des membres, l'arthrose et une mobilité réduite.
Un diagnostic et une prise en charge appropriés des affections de la hanche nécessitent une compréhension approfondie de l'anatomie, de la fonction et des pathologies potentielles de l'articulation. Une combinaison d'examen clinique, d'imagerie (radiographie, IRM) et d'arthroscopie peut contribuer à un diagnostic précis. Les options thérapeutiques peuvent inclure :
Penses-tu tout connaître de ce cours ? Ne tombe pas dans les pièges, entraine-toi à l'aide des QCM ! eBiologie recense des centaines de questions pour t'aider à maîtriser ce sujet.
Découvrez les peroxysomes, des petits organelles cellulaires clés pour la survie et l'adaptation de nos cellules ! À travers ce cours de biologie cellulaire, vous ex...

Découvrez comment notre ADN se reproduit à chaque cellule division dans ce cours de biochimie moléculaire : « Réplication du DN ». Vous apprendrez les étapes clés de...
Découvrez la biologie du développement évolutif, le domaine qui étudie les mécanismes du développement embryonnaire et leur évolution au niveau moléculaire, cellulai...