Arthrology, or syndesmology
course-show.h1-title
Delving into the study of human joints, this course will introduce you to the hip joint, a key component of the musculoskeletal system. We'll explore the structures that make it up and the movements it enables. We'll also develop our understanding of the pathologies that can affect this crucial joint.
Introduction
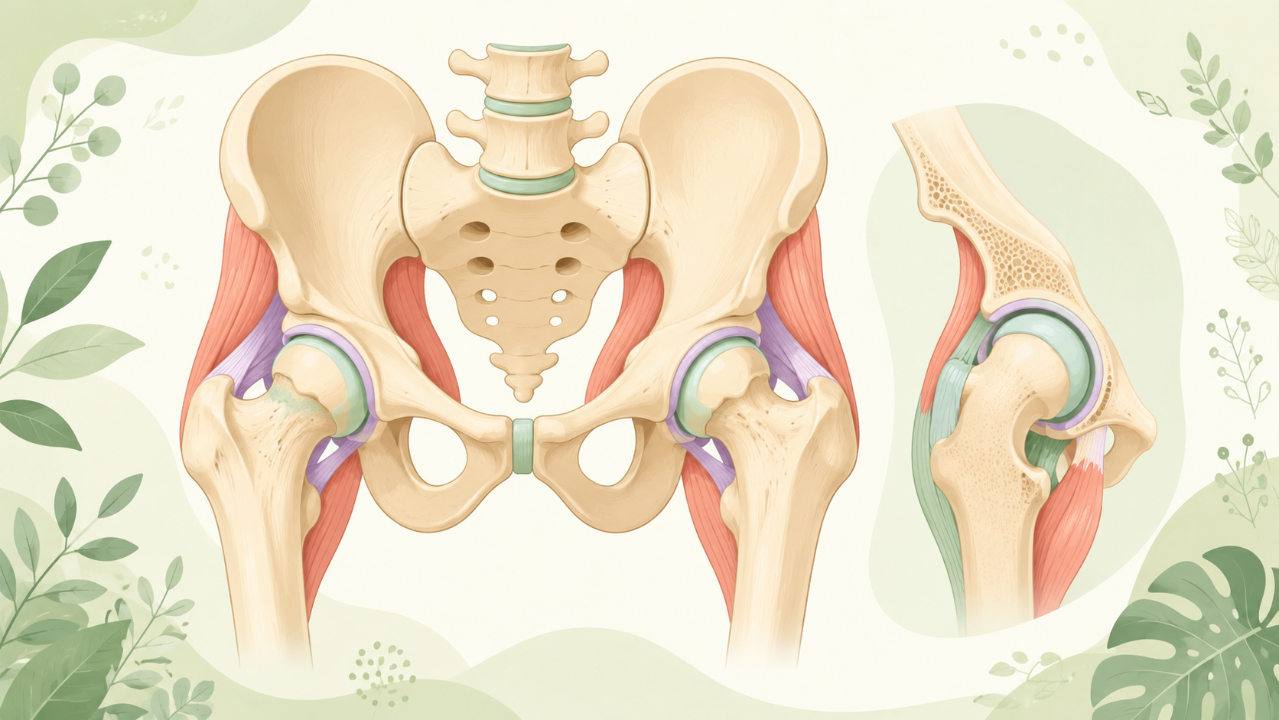
The hip joint, or coxal-femoral joint, is one of the largest and most robust synovial joints in the human body. It serves as a ball-and-socket joint connecting the pelvis (acetabulum) to the femur (head). The hip joint enables a wide range of movements, including flexion, extension, abduction, adduction, internal rotation, and external rotation. This article provides an in-depth exploration of the anatomy, development, biomechanics, pathologies, and clinical considerations related to the hip joint.
Anatomy
Bony Landmarks
The bony elements forming the hip joint include the acetabulum (part of the pelvis) and the femoral head. The acetabulum is a deep cup-shaped cavity formed by the ilium, ischium, and pubis. The femoral head is the rounded end of the femur located above the neck.
Articular Surfaces
The articular surface of the acetabulum is lined with hyaline cartilage that covers the bony cavity's labrum. The articular surface of the femoral head is also covered by hyaline cartilage, which articulates with the acetabular labrum and socket.
Ligaments
Several ligaments provide stability to the hip joint, including:
- Iliofemoral ligament: Connects the ilium and femur and limits abduction.
- Pubofemoral ligament: Connects the pubis and femur and limits adduction.
- Ischiofemoral ligament: Connects the ischium and femur and provides additional stability during abduction.
- Labral ligament complex (acetabular labrum): This fibrocartilaginous structure surrounds the acetabulum's articular surface, deepening the socket and providing a seal against joint laxity.
Development
The hip joint develops from three embryonic tissues: the somatic mesoderm, sclerotome, and lateral plate mesoderm. By the end of week 5, the lower limb bud appears as an outgrowth from the caudal end of the body. The femur and pelvis differentiate and form the hip joint during the following weeks.
Biomechanics
The hip joint's range of motion is essential for locomotion, posture maintenance, and other daily activities. The primary muscles responsible for hip movements are:
- Iliopsoas: Flexes, adducts, and internally rotates the hip.
- Gluteus maximus: Extends, abducts, and externally rotates the hip.
- Gluteus medius and minimus: Abducts and stabilizes the hip during walking and running.
- Tendinous insertion of rectus femoris: Flexes and internally rotates the hip during knee extension.
Pathologies
Hip Joint Injuries
Injuries to the hip joint can result from falls, sports-related accidents, or high-impact activities. Common injuries include:
- Labral tears: These often occur due to repetitive stress or acute trauma and may cause pain, clicking, or locking of the joint.
- Femoral head and neck fractures: These can result from severe trauma and may lead to osteoarthritis if not treated promptly.
- Dislocations: Hip dislocations are rare but can be caused by high-energy traumas such as motor vehicle accidents or falls from a height.
Osteoarthritis
Osteoarthritis (OA) is the most common joint disorder, characterized by degeneration of articular cartilage, subchondral bone changes, and osteophyte formation. Risk factors for developing hip OA include aging, obesity, genetics, and previous joint injuries.
Developmental Dysplasia of the Hip (DDH)
DDH is a congenital or developmental disorder characterized by an unstable hip joint due to abnormal acetabular development. Early detection and treatment are crucial to prevent further complications such as limb length discrepancy, osteoarthritis, and reduced mobility.
Clinical Considerations
Proper diagnosis and management of hip-related disorders require a thorough understanding of the hip joint's anatomy, function, and potential pathologies. A combination of clinical examination, imaging modalities (X-ray, MRI), and arthroscopy can help in making an accurate diagnosis. Treatment options may include:
- Conservative management: Rest, physical therapy, and medication for pain relief.
- Arthroscopic surgery: Minimally invasive procedure to treat labral tears, chondral lesions, or loose bodies within the joint.
- Open surgery: For more extensive damage, such as femoral head and neck fractures or dislocations, open surgical intervention may be necessary.
- Joint replacement: In severe cases of osteoarthritis or degenerative joint disease, total hip arthroplasty (THA) can provide significant pain relief and improved mobility.